
Splanchnic Ultrasound to Guide Unloading in VA-ECMO
Keywords:
Cardiogenic shock - Unloading - Cardiac and Abdominal ultrasoundAbstract
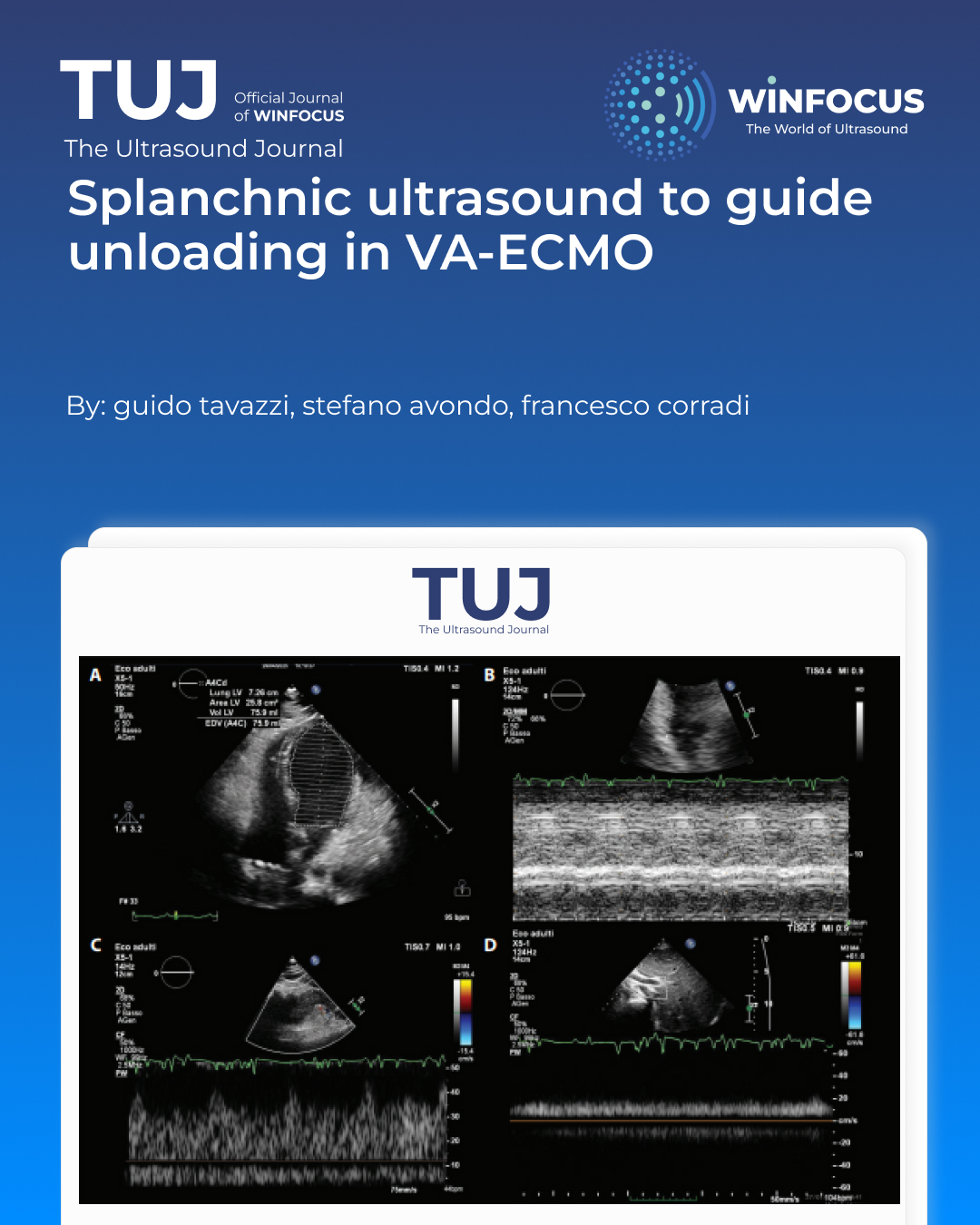
Patients supported with veno-arterial extracorporeal membrane oxygenation (VA-ECMO) may require left ventricular (LV) unloading to prevent pulmonary congestion and adverse hemodynamic interactions. However, defining the need and timing of unloading remains challenging, as current approaches rely predominantly on cardiac and pulmonary parameters, often neglecting systemic and organ-level congestion. We report the case of a 53-year-old woman admitted with cardiogenic shock following pericardial drainage and mediastinal mass biopsy. Due to rapid hemodynamic deterioration, VA-ECMO was initiated, resulting in stabilization. Early echocardiographic assessment showed severe biventricular dysfunction but evidence of partial aortic valve opening without LV distension. To further characterize the hemodynamic profile, splanchnic Doppler ultrasound was performed, demonstrating preserved renal arterial flow (resistive index <0.72), continuous intrarenal venous flow, and low portal vein pulsatility (<30%), consistent with a non-congestive phenotype. Based on this integrated assessment, LV unloading was deferred. Subsequent pulmonary artery catheterization confirmed low filling pressures despite reduced cardiac output. A diagnosis of stress-induced cardiomyopathy was suspected, and levosimendan was administered, leading to rapid improvement in cardiac function and successful ECMO weaning. Final pathology revealed a thymic neuroendocrine carcinoma. This case highlights the limitations of relying solely on cardiac indices to guide LV unloading decisions during VA-ECMO. Splanchnic Doppler provided a non-invasive, real-time evaluation of the perfusion–congestion balance at the organ level, complementing echocardiographic and invasive hemodynamic data. The integration of multimodal monitoring may allow a more comprehensive understanding of patient–device interaction and support individualized management strategies. Further research is needed to validate the role of splanchnic ultrasound in guiding unloading decisions and optimizing outcomes in patients with cardiogenic shock supported by VA-ECMO.
References
1. Ezad SM, Ryan M, Donker DW, Pappalardo F, Barrett N, Camporota L, et al. Unloading the Left Ventricle in Venoarterial ECMO: In Whom, When, and How? Circulation. 2023 Apr 18;147(16):1237-50. PubMed PMID: 37068133. Epub 20230417.
2. Corradi F, Bell M, De Rosa S. Kidney Doppler ultrasonography in critical care nephrology. Nephrol Dial Transplant. 2024 Aug 30;39(9):1416-25. PubMed PMID: 38697934.
3. Mariani S, Richter J, Pappalardo F, Belohlavek J, Lorusso R, Schmitto JD, et al. Mechanical circulatory support for Takotsubo syndrome: a systematic review and meta-analysis. Int J Cardiol. 2020 Oct 1;316:31-9. PubMed PMID: 32473281. Epub 20200528.
4. Schrage B, Becher PM, Bernhardt A, Bezerra H, Blankenberg S, Brunner S, et al. Left Ventricular Unloading Is Associated With Lower Mortality in Patients With Cardiogenic Shock Treated With Venoarterial Extracorporeal Membrane Oxygenation: Results From an International, Multicenter Cohort Study. Circulation. 2020 Dec;142(22):2095-106. PubMed PMID: 33032450. Pubmed Central PMCID: PMC7688081. Epub 20201009.
5. Tavazzi G, Spiegel R, Rola P, Price S, Corradi F, Hockstein M. Multiorgan evaluation of perfusion and congestion using ultrasound in patients with shock. European Heart Journal: Acute Cardiovascular Care. 2023;12(5):344-52.
6. Verbrugge FH, Guazzi M, Testani JM, Borlaug BA. Altered Hemodynamics and End-Organ Damage in Heart Failure: Impact on the Lung and Kidney. Circulation. 2020 Sep 8;142(10):998-1012. PubMed PMID: 32897746. Pubmed Central PMCID: PMC7482031. Epub 20200908.
7. Corradi F, Tavazzi G. The Doppler combined assessment of splanchnic perfusion and congestion in cardiogenic shock: a physiological approach. Intensive Care Med. 2025 Jun;51(6):1168-71. PubMed PMID: 40140096. Epub 20250326.
8. Maddox DAD, W.M.; Brenner, B.M. Handbook of Physiology. Renal Physiology; American Physiological Society: Bethesda, MD, USA1992.
Downloads
Issue
Section
License
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Authors retain the copyright for their published work. No formal permission will be required to reproduce parts (tables or illustrations) of published papers, provided the source is quoted appropriately and reproduction has no commercial intent.
How to Cite









